

By Matt Stanlake — Head Physiotherapist & Director, Upwell Health Collective. APA Member. AHPRA Registration: PHY0000975408. 20 years clinical experience. Last reviewed: May 2026.
Reading time: approximately 75 minutes. This is a long-form clinical monograph for patients, athletes, parents, coaches, and clinicians who want to understand ACL recovery deeply — not in headlines.
This is a Whole Person Care monograph.
The Atlas you are about to read uses ACL recovery as its worked example — because the ACL is one of the highest-stakes injuries in sport, and every clinical system has to come back online for the athlete to return well. But the framework you'll learn here works for any condition you treat.
Whole Person Care™ is a clinical operating system. Hardware. Software. Energy Plant. Autonomic Nervous System. It is the way every system in the body either supports or undermines recovery — and the way clinicians can read those signals in the room.
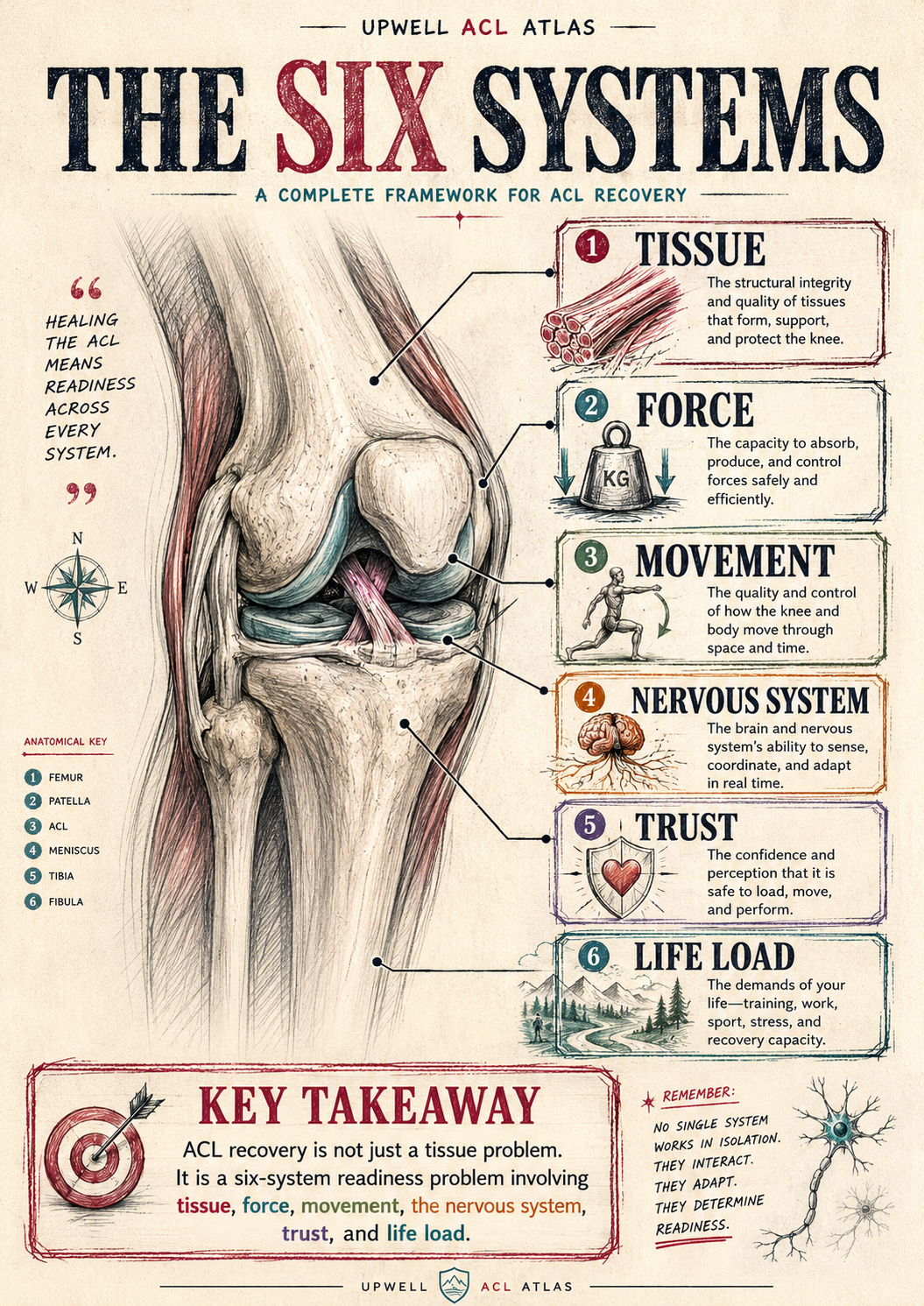
The 6-System ACL Framework is what happens when you apply Whole Person Care to the most demanding return-to-sport injury in modern physiotherapy. Tissue. Force. Movement. Nervous System. Trust. Life Load. Read the ACL specifics if you're treating one. Read the framework if you're a clinician. Most of you will do both.
The Atlas does not believe that any single system — tissue, neural, mechanical, behavioural — recovers athletes alone. It assumes the opposite. It assumes you came here to do the harder, better, more accurate work.
For the clinician reading this: If you take one thing from this monograph, take the operating system. The ACL is the example. The method is the gift. Apply it to the next chronic pain patient, the next tendinopathy, the next post-op shoulder. You'll find the same questions hold across the body. That's the whole point.
— Matt · Founder, Whole Person Care™
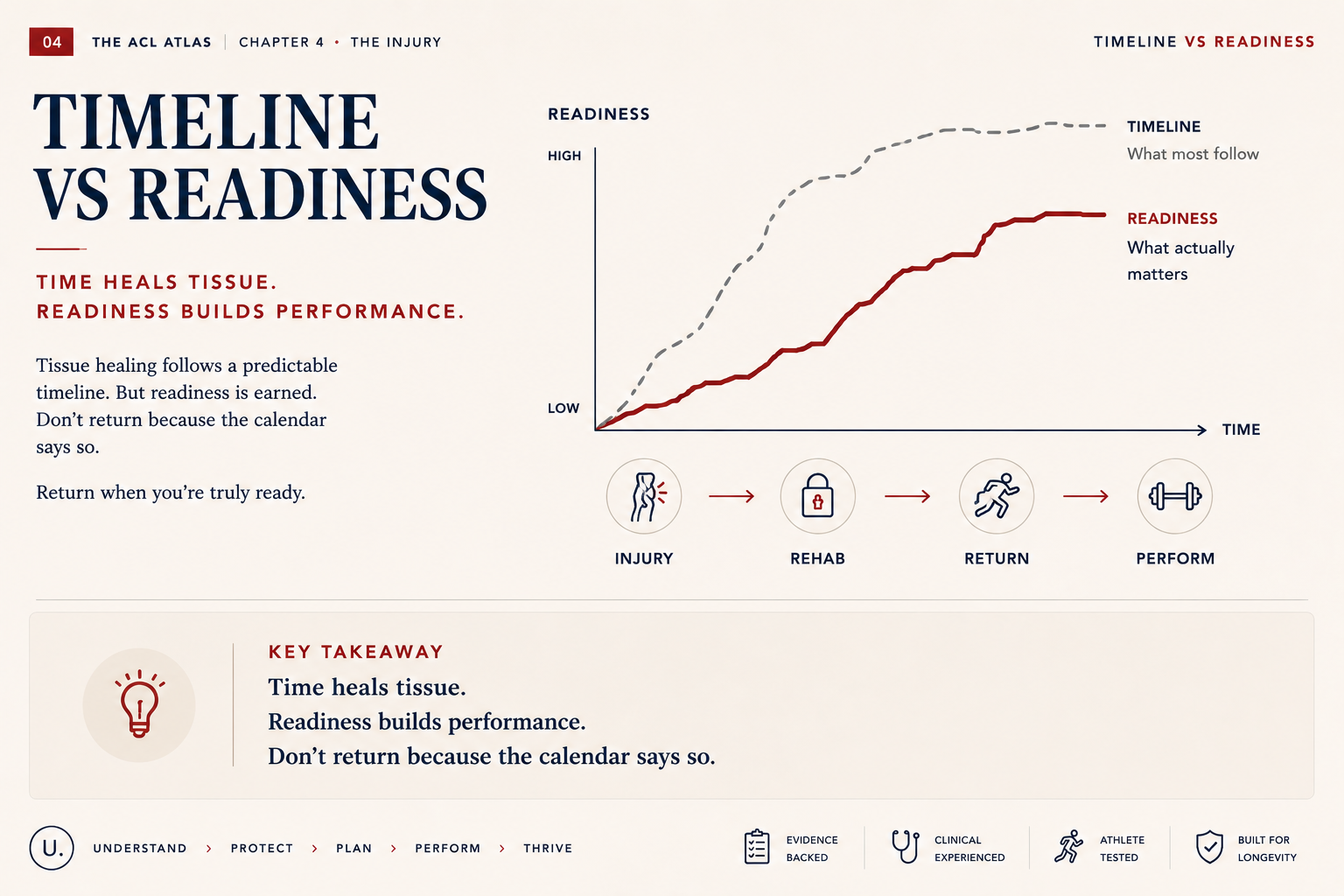
Most ACL education hands you a timeline. Injury. MRI. Surgeon. Surgery. Six weeks. Three months. Six months. Nine months. Run. Hop. Play. It looks tidy on paper. It rarely plays out that way in clinic.
I've spent twenty years rehabbing knees. The athletes who return well — who actually trust the knee at full pace, in chaos, under fatigue, against an opponent — are not the ones who ticked the calendar. They're the ones whose tissue, force, movement, nervous system, trust and life load all caught up to each other at the same time. That's the gap this Atlas exists to close. Not another guide that tracks the calendar. A system that asks a different question.
What the timeline asks: Are you healing? How many months since surgery? Is the graft old enough? Can you straighten the knee? Has the swelling gone? Can you run? Can you hop? Did the surgeon clear you?
What readiness asks: Are you ready? Can you absorb force at full speed? Can you brake under fatigue? Can you react when the play breaks down? Has the brain remapped the knee? Do you trust it under pressure? Can you recover between bouts? Does the rest of your life have room for this?
One question tracks healing. The other tracks readiness. The standard pathway stops at the first. The Atlas starts with the second.

The problem isn't that the old model is useless. It's that it stops measuring before the athlete is actually ready.
Standard ACL rehab tracks the things that are easy to measure: pain, swelling, range of motion, a strength number, a hop test, a date on a calendar. These are useful. They tell you the knee is healing.
But sport doesn't ask any of those questions. Sport asks whether you can decelerate from a sprint with a defender on your shoulder. Whether you can land from a contested ball with one leg under you. Whether you can reorganise mid-air when the play breaks down. Whether you'll choose to plant the leg when the moment matters — or hesitate. None of that shows up on a hop test. None of that shows up on a calendar.
Key takeaway: These markers tell you if you're healing. They don't always tell you if you're ready.
The Atlas exists to fill that gap. Not by replacing the standard pathway — by adding the layers it doesn't see. Force speed. Deceleration. Reactive agility. Nervous system control. Trust. Fatigue. Life load. Long-term knee health. That's what the next module is about: the framework Upwell uses to organise all of it. The lens we use to think about human recovery — and the map we use to apply it to ACL.
From Whole Person Care™ to Whole Athlete Care.
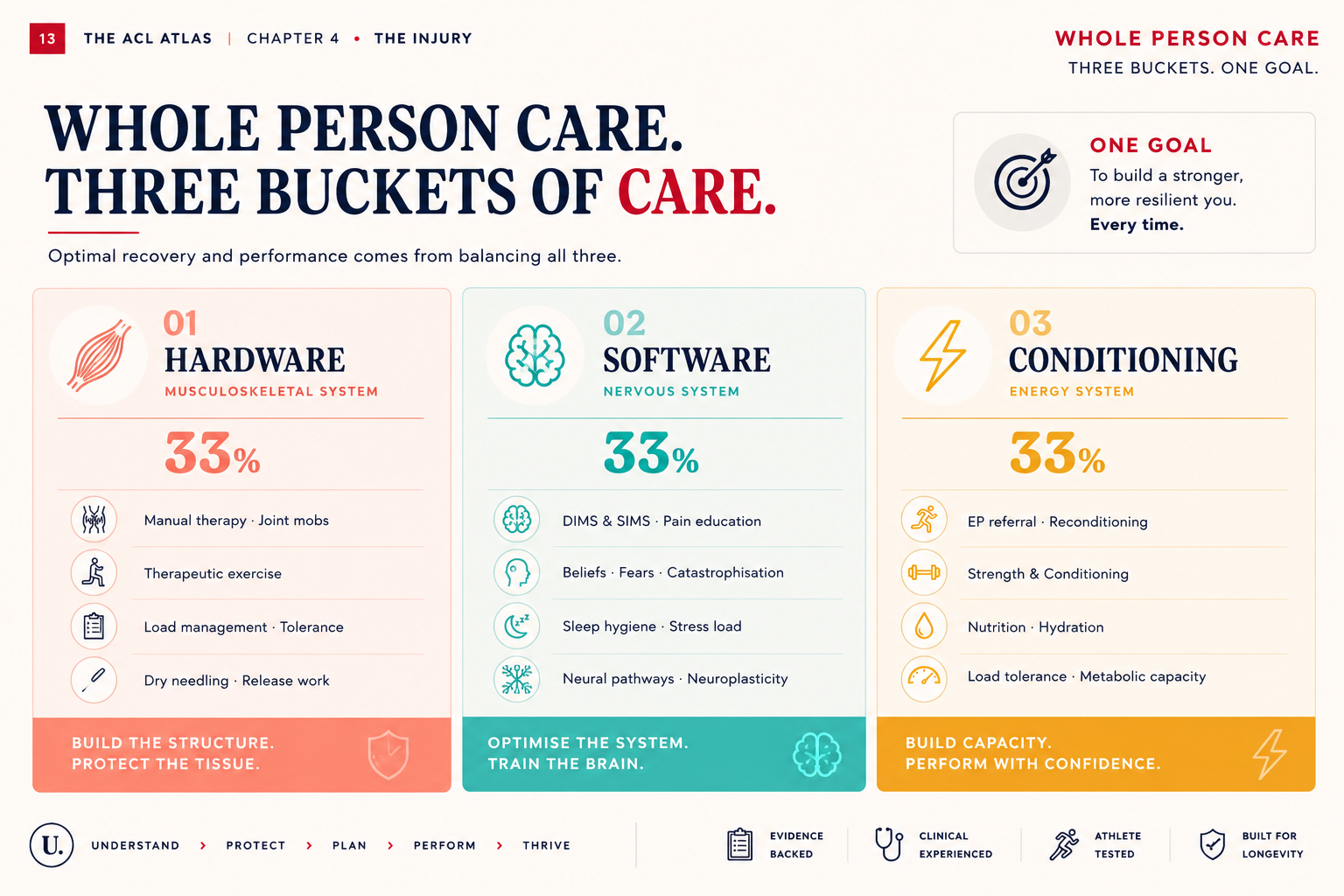
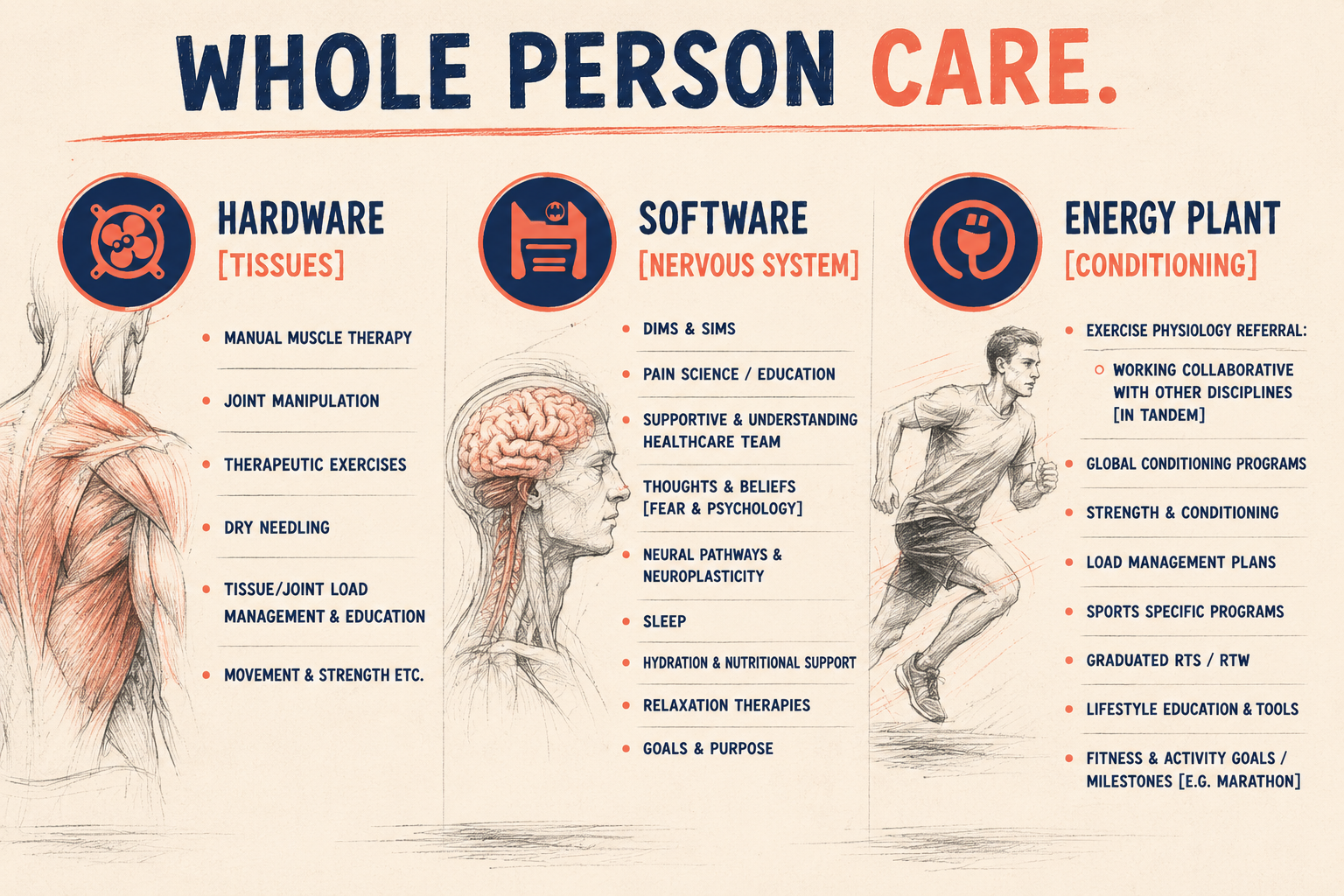
Every patient walks in with three buckets to fill.
Hardware — the tissue, the joint, the graft, the muscle, the bone, the physical structures that orthopaedics has spent a century learning to repair. Hardware is what the surgeon fixes. It is real, it is measurable, and it is necessary.
Software — the nervous system, the threat response, the beliefs, the fears, the patterns, the autonomic state, the trust the brain holds in the body. Software is what the surgeon cannot fix. Software is what most rehabilitation systems quietly ignore.
Energy Plant — the daily metabolic, hormonal, and life-load capacity that determines whether either of the above can actually adapt. Sleep, nutrition, stress, recovery, life context. Without it, nothing else lands.
You cannot rehabilitate Hardware without Software. You cannot return an athlete to elite sport with a beautifully reconstructed knee and a nervous system that still thinks the leg is going to collapse. Both spines have to be rebuilt — and the Energy Plant has to be online to support both. That is Whole Person Care.
Hardware. Software. Energy Plant. The interventions live inside the buckets — not above them. A patient who needs Energy Plant support but is given more Hardware work plateaus. A patient who needs Software training but is given heavier loads plateaus. The bucket diagnosis is the unlock.
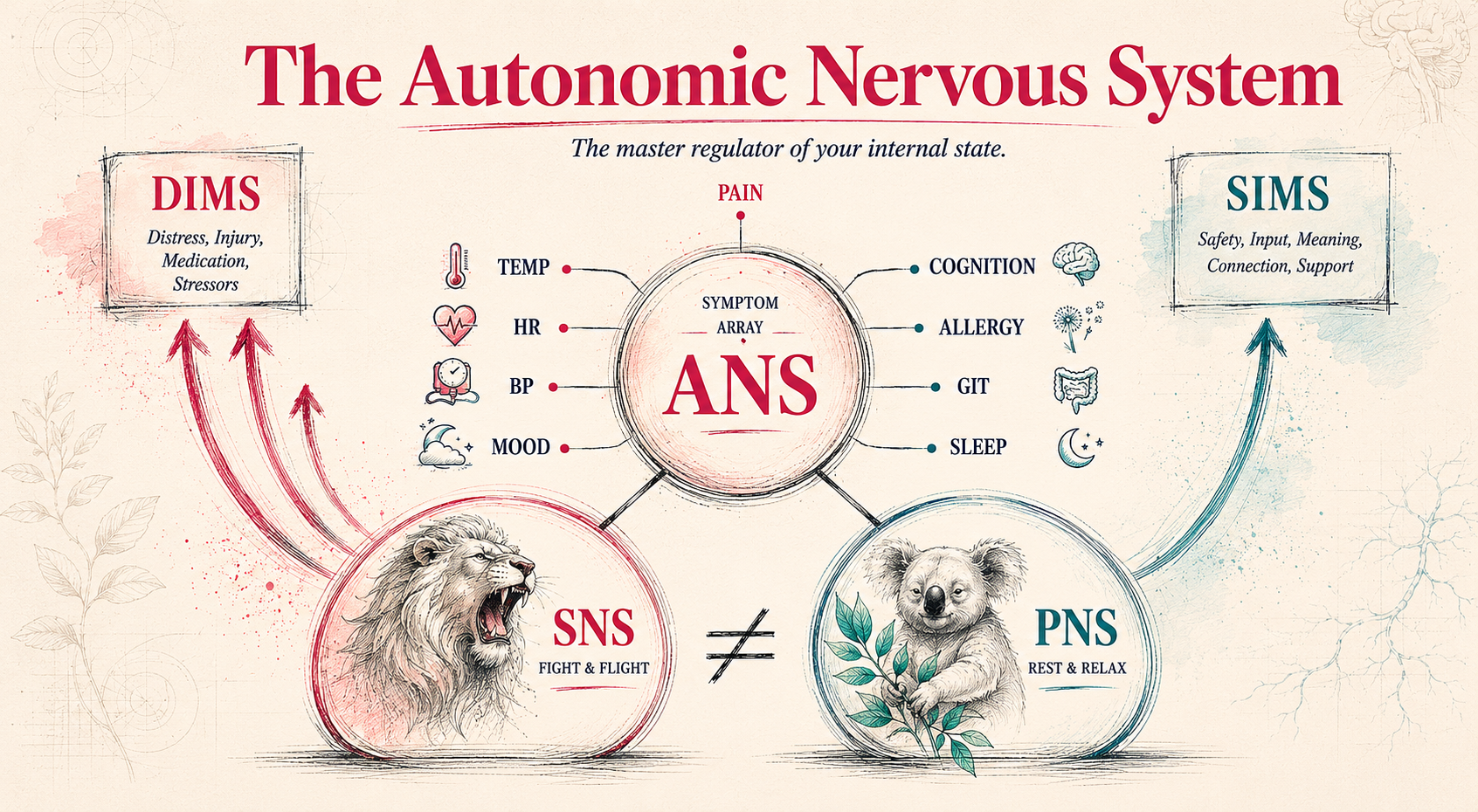
The autonomic nervous system is the fourth bucket — and the one most clinicians never name.
The Lion is sympathetic — fight, flight, vigilance, threat. The Koala is parasympathetic — rest, digest, repair, sleep. Healing happens in Koala. Performance happens in Lion. The athlete who can't move between them does not recover — no matter how strong the quad gets. Cortisol does not care about your hop test. One of the most underrated rehab interventions is the one that gets the patient back into Koala long enough for tissue to repair, for sleep to consolidate motor learning, for the threat response to settle. Without it, every gain is built on sand.
Whole Person Care™ gives us the lens. Above The Ceiling gives us the ACL map. Whole Athlete Care is what happens when that philosophy meets sport injury.
The bridge: The six systems are not six boxes. They're six dials on the same mixing desk — and moving one always moves the others.
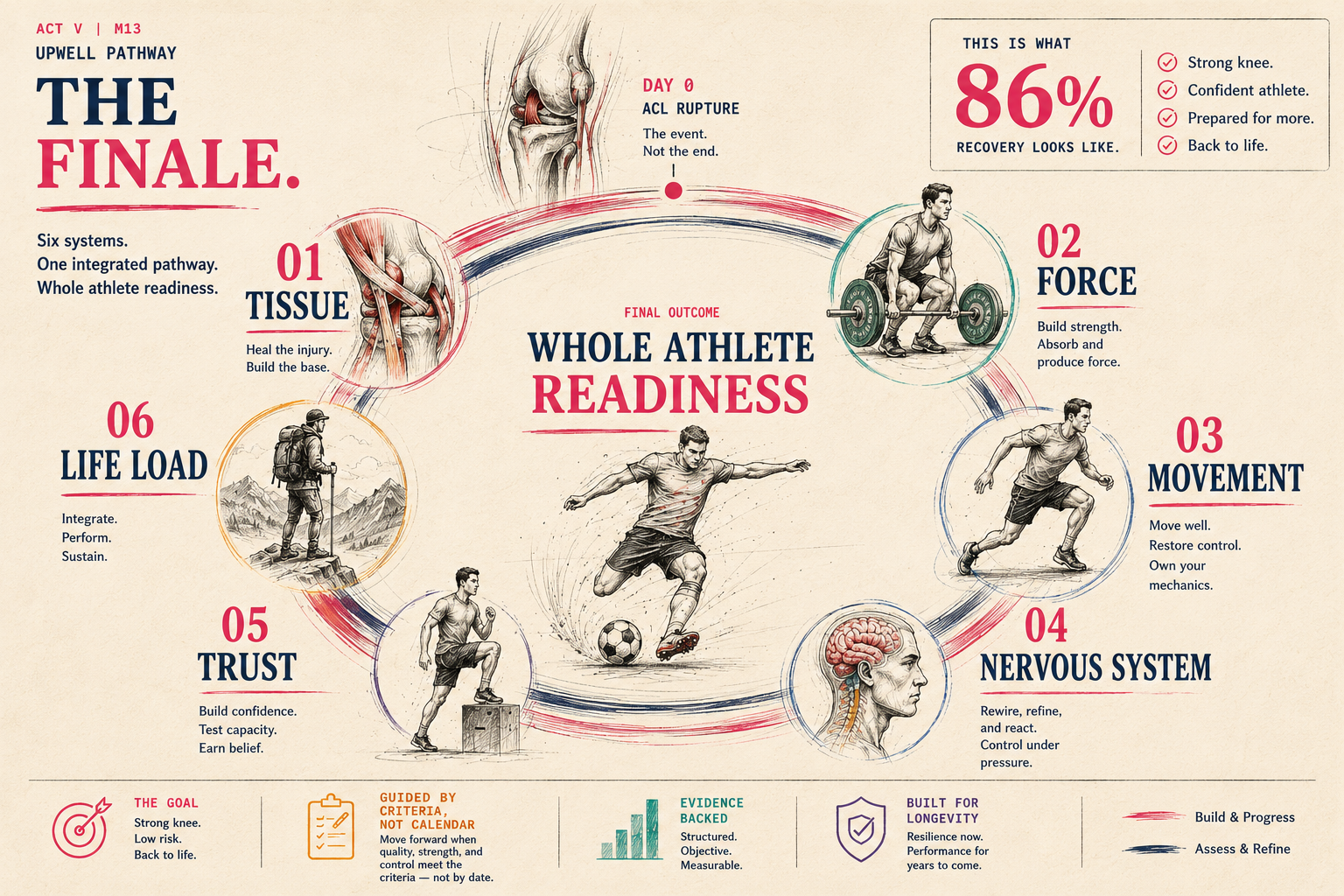
We organise ACL recovery through six systems. Not because it sounds clever. Because athletes don't return to sport as isolated knees — they return as whole humans under load, pressure, fatigue, uncertainty and chaos. Each system below is a separate chapter further down. Together, they're how Upwell decides if an athlete is actually ready.
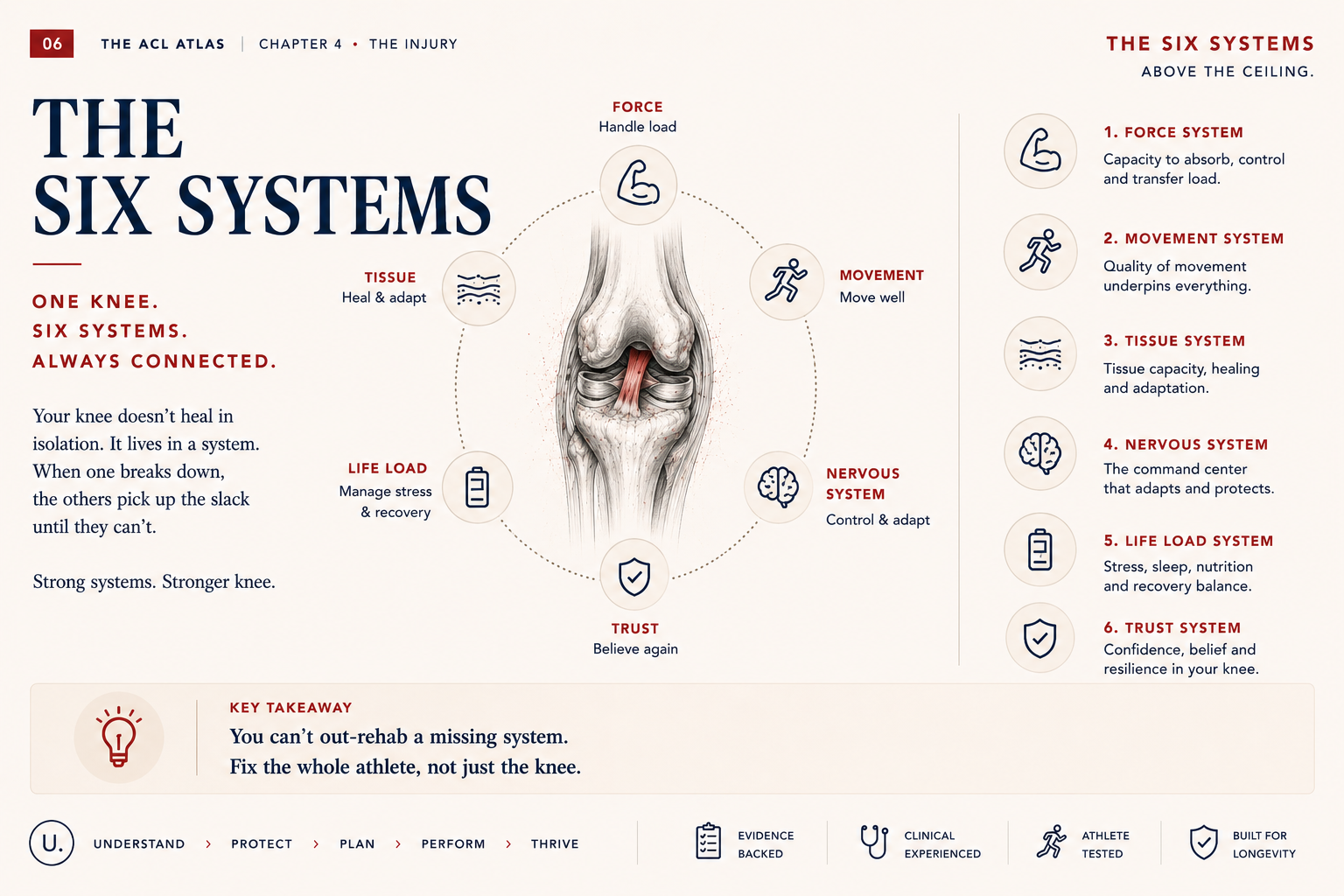
01 — Tissue. The biological foundation. Common failure: pain-free is mistaken for healed. Biology moves slower than symptoms. Readiness asks: has the biology actually caught up with how the knee feels?
02 — Force. The engine of performance. Common failure: strong in the gym, slow to produce force when sport actually asks. Readiness asks: can force be produced, absorbed and repeated at sport speed?
03 — Movement. The skill of control. Common failure: looks textbook at slow speed, falls apart when the play breaks down. Readiness asks: can the knee land, brake, cut and react when sport stops being scripted?
04 — Nervous System. The command centre. Common failure: the knee heals, but the brain's map of the knee never gets redrawn. Readiness asks: has the nervous system relearned the knee — under speed, fatigue and decision load?
05 — Trust. The belief to perform. Common failure: the body is ready, the athlete isn't. Hesitation is its own injury risk. Readiness asks: does the athlete actually trust the knee when the pressure is real?
06 — Life Load. The daily context of recovery. Common failure: same program, different cost. Rehab doesn't happen in a vacuum. Readiness asks: does the rest of life — sleep, work, stress, school — leave room for recovery to land?
The integration: Six dials. One recovery. Tissue limits force. Force shapes movement. Movement teaches the nervous system. The nervous system changes trust. Trust changes output. Life load changes capacity across every system. Move one dial — the others move with it.
Biology heals on its own clock — and the clock does not care how the knee feels.
The first thing I tell every ACL patient is this: your knee feels better long before your knee is better. That gap between "feels good" and "is actually ready" is where most re-injuries live. Tissue healing has its own timeline. Graft maturation. Bone tunnel integration. Cartilage adaptation. Meniscus repair. None of these care about how confident you feel walking up stairs at week six. They take the time they take.
A reconstructed ACL graft weakens before it strengthens. It is biologically weakest between weeks 6 and 12 — exactly when symptoms feel best.
Think of your new ACL like a house renovation. On day one, the new beam is in place — but the walls haven't been rebuilt around it yet. It takes the body 9 to 12 months to fully rebuild the structure around the graft. The first 6 to 12 weeks, the graft is at its weakest as your body integrates it. Then it slowly gets stronger. The knee feeling good is not the same as the knee being done.
Graft remodelling follows three phases: early inflammatory necrosis (0–4 wks), proliferation and revascularisation (4–12 wks), and ligamentisation (3–12+ months). Mechanical strength drops during phase two as the graft becomes hypocellular before recovering tensile properties. Concurrent meniscal repair extends loading restrictions by 6–12 weeks depending on tear location. Bone tunnel widening peaks at 3–6 months. Biology, not protocol, sets the floor.
Treating "no pain" as "ready to load." Pain has resolved well before tissue is mechanically ready. The athlete pushes hard, biology hasn't caught up, the knee responds with swelling 24–48 hours later.
Ignoring concurrent meniscus or cartilage status. The ACL gets all the attention. The meniscus repair quietly sets the loading ceiling. Heavy impact too early stresses the repair, not the graft.
Skipping the early loading window. The opposite mistake. Tissue adapts to load. Going too soft for too long means the tissue never builds the capacity it needs.
Forgetting the rest of the system. Sleep, protein intake, training stress, life stress — all change healing speed. We see athletes plateau on rehab and the answer turns out to be in their week, not their program.
We track tissue readiness as a separate system, never as a default of "weeks since surgery."
Key takeaway — Tissue. The knee feels better long before the knee is better. Biology runs on its own clock and we plan against it, not around it. When tissue is respected, the rest of the system gets a fair chance. Start here. Every time.
Clinical note: "The graft you reconstruct on Monday is not the graft you load on Friday. Biology is doing work you can't see." — Matt · 20 yrs in clinic
Watch for: Concurrent meniscus repair quietly sets the ceiling on impact loading for the first 12 weeks. Always check the op report.
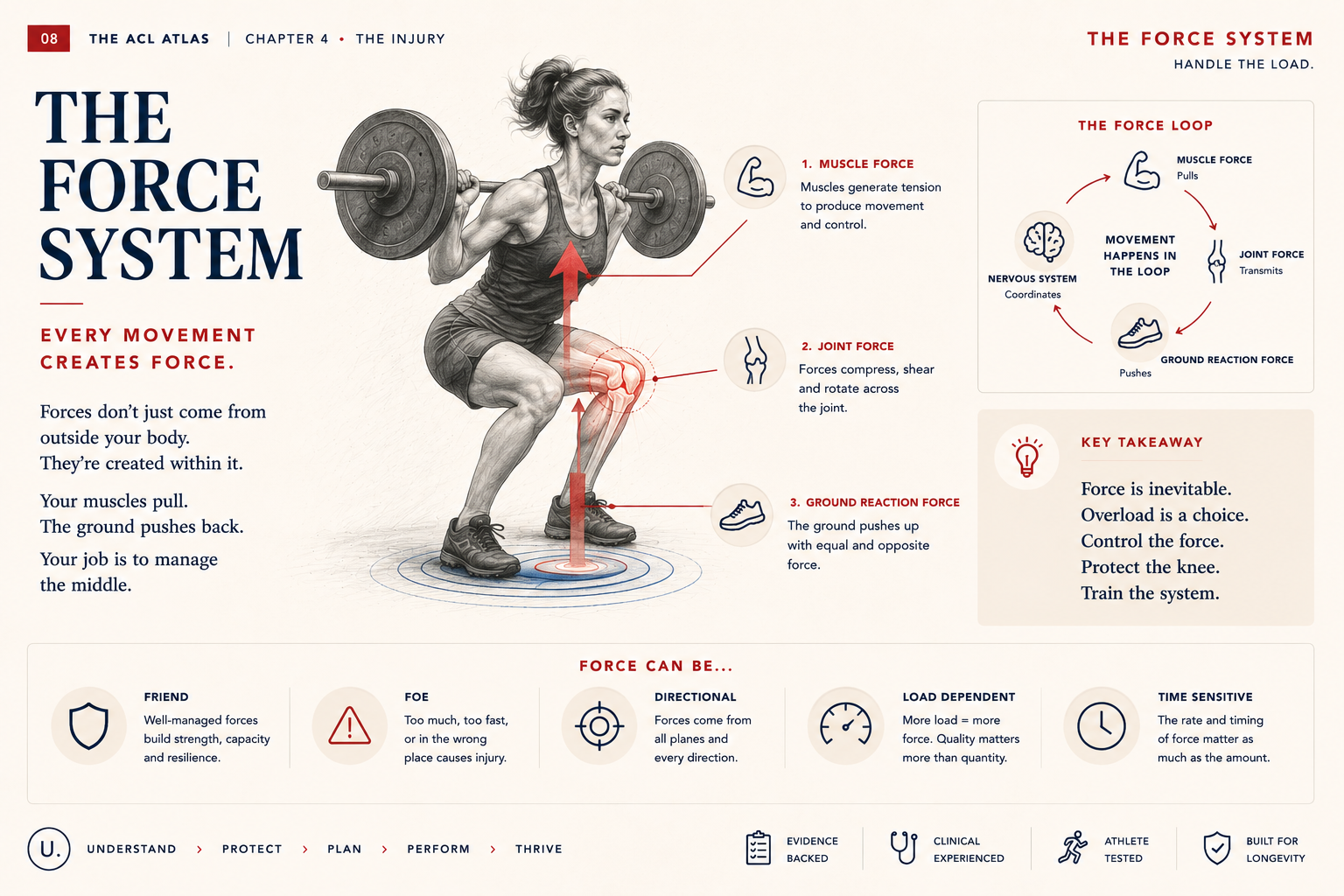
Strength is not force. And force is not output. Sport runs on output.
The strongest athletes I rehab are rarely the slowest to return. They're often the slowest to be ready. Big numbers in the gym don't always translate to fast force on the field — and the gap between the two is where ACL re-injury hides. Sport doesn't ask you to push 1.5 times bodyweight at a slow grind. It asks you to produce, absorb and re-direct force in tenths of a second, hundreds of times in a row, under fatigue, while reading an opponent.
Strength rebuilds first. Rate of force development rebuilds last — and sport demands the second one, not the first.
You can leg-press a house and still be the slowest one off the line. Strength is how much you can lift. Force on the field is how fast you can hit a number — not how big the number is. ACL recovery rebuilds slow strength first. Sport speed has to be trained on top of that. Skip the second half and you go back to sport with a strong knee that's not yet ready.
Isokinetic quad strength typically normalises 6–9 months post-op in compliant athletes. RFD at 100ms, eccentric quad capacity, and reactive strength index commonly remain >15% deficit at 12+ months in the same cohort. LSI on slow tests overestimates readiness. Force-plate metrics (CMJ asymmetry, eccentric deceleration, propulsive impulse) catch the gap that isokinetic numbers miss.
Clearing on slow strength alone. 90% LSI on a leg press or isokinetic test is the floor, not the ceiling. Without force-plate or jump-test data, the athlete returns with hidden deficits.
Skipping eccentric and deceleration loading. Concentric strength is straightforward to build. Eccentric force absorption — landing, braking, redirecting — needs its own dedicated phase, and rarely gets one.
No reactive / fast-twitch work. Sport asks for force in 100–200 ms windows. If the program never trains that window, the athlete returns to sport with a slow nervous system attached to a strong leg.
Symmetry hides imbalance. Both legs can be equally weak. LSI looks great. The athlete returns underprepared on both sides, not just the involved side.
Objective force-plate testing through every phase. We don't return-to-sport on a single number — we return on a profile.
Key takeaway — Force. Slow strength is the floor. Force at sport speed — and the ability to absorb it — is what readiness actually asks. Strength gets us into the room. Force gets us back on the field.
VALD note: CMJ asymmetry >10% at 9 months is one of the strongest single-metric predictors of poor return-to-sport outcome.
Watch for: Eccentric decel testing is the cheapest way to find athletes who will fail a cutting test before you let them cut.
Quality at slow speed is the warm-up. Quality at full speed, in chaos, is the work.
I've watched dozens of athletes pass a textbook single-leg squat then fall apart the moment a ball is thrown into the drill. The slow-motion knee is not the sport knee. The body knows the difference even when the test doesn't. Movement isn't a single quality. It's a stack — landing, decelerating, cutting, reacting, recovering from a missed step, deciding which leg to plant. Each layer needs its own time, its own load, and its own honest test.
Clean movement at slow, predictable speed is the baseline. Clean movement at sport speed, under decision load and fatigue, is the target.
A clean squat in the mirror is a starting point, not a finish line. The question that matters is: does your knee still move that well when you're tired, surprised, off balance, and the play has changed? We rebuild movement quality the same way you learned to drive. Empty car park first. Quiet roads next. Then traffic. Then traffic at night, in the rain, with someone yelling at you. Same knee, totally different demand.
Movement quality drops under three predictable contexts: speed, fatigue, and cognitive load. ACL re-injury mechanism studies consistently show breakdown under at least one of these — most often two or three at once. Linear progressions from open-chain to closed-chain to plyometric are necessary but not sufficient. Reactive, unanticipated, dual-task and fatigued testing belong on every clearance protocol.
Clearing on scripted hop tests alone. Single, double, triple, crossover hop — all predictable. They prove a baseline. They don't prove sport readiness.
Never testing under fatigue. Quality at minute one and quality at minute forty are different sports. If you don't test fatigued, you don't know.
Skipping reactive and unanticipated cuts. Pre-planned change of direction is the easy version. Reactive, last-moment cuts produce the loads that injured the ACL in the first place.
Cognitive load left out of testing. Add a decision — a ball, a call, a defender — and movement quality drops. If you've never tested that drop, you've never tested sport.
"Looks good to me" is not a metric. Eyeballing knee control is unreliable across clinicians. Video, force plate, and structured criteria all beat the human eye on tired Thursdays.
We progress movement through three layered demand contexts — speed, fatigue, decision — and only clear when the knee holds across all three.
Key takeaway — Movement. The knee has to move well under speed, under fatigue, and under decision load — not just in front of a clinician on a Tuesday morning. Sport doesn't reward the clean squat. It rewards the athlete whose knee holds when everything else is breaking down. That is what we train for.
Mechanism note: Most non-contact ACL injuries occur within 50 ms of foot strike — well below conscious correction time. Pattern, not effort.
Watch for: Trunk lean, hip drop, dynamic valgus on the third repetition of a decel cut, not the first. Fatigue is the test.
When the ACL ruptures, the brain's map of the knee breaks. Surgery rebuilds the ligament. It does not rebuild the map.
Here's a thing most athletes don't know: an ACL injury is a brain injury as much as it is a knee injury. Not in the concussion sense. In the map sense. The detailed, automatic, millisecond-by-millisecond model your brain holds of where the knee is, what it's doing, and how to defend it — that map goes offline at the moment of rupture, and it does not come back on its own.
I've worked with athletes who passed every strength test, every hop test, every clearance criterion — and still couldn't plant the leg under pressure. Their knee was strong. Their nervous system was still rebuilding the map.
The ACL is not just a ligament. It is a sensory organ. When it ruptures, the brain loses a primary input channel — and the loss persists long after the graft is healed.
Before the injury, your brain knew exactly where your knee was without you having to think about it. That sense was built from thousands of tiny sensors inside the ligament — and those sensors are gone now. The brain rebuilds that sense by collecting new evidence — from the muscles around the joint, from balance, from vision, from movement. Rehab is how we feed it that evidence. The longer and more varied the training, the better the new map.
Loss of mechanoreceptor input from the ruptured ACL drives sustained central reorganisation. Imaging studies show increased motor cortex activation, reduced sensorimotor cortex activation, and increased visual-motor coupling at 12+ months post-op. Outputs to train: reactive balance, unanticipated cutting, dual-task gait, visual-occlusion drills, and external-focus cueing. Closed-eyes single-leg balance is the floor — not the ceiling.
Treating proprioception as a balance-pad warm-up. Two minutes on a wobble board doesn't rebuild a sensory map. The brain needs varied, unpredictable, repeated input across thousands of contacts.
Skipping the visual-system layer. Most athletes lean on vision to compensate for lost proprioception. If you never train them with vision restricted or distracted, the deficit stays hidden until match day.
No dual-task or cognitive-load training. Motor planning under cognitive load is where injuries happen. Tested on its own, the knee looks fine. Tested with a decision attached, the truth shows up.
Forgetting the uninvolved side. The opposite knee also rewires after an ACL rupture. If you only train the involved side, you leave half the nervous system underprepared.
We train the brain to trust the knee again — through evidence, repetition, and progressively unpredictable contexts.

Key takeaway — Nervous System. The ligament heals on a timeline. The map heals on a workload. Strong knees with poor maps are still un-ready knees. Test it honestly. Or watch it fail on match day.
Imaging note: fMRI studies post-ACLR show persistent shifts in motor cortex activation and visual-motor coupling well past 12 months. The brain is doing work the strength test can't see.
Watch for: Athletes who look down at the knee mid-task. Watching is a tell that vision is doing the work proprioception should be doing.
The last system to come back. The first system to break sport.
I've had athletes pass every objective test we can throw at them — and then sit on the bench at the moment of truth, because the body was ready and the athlete wasn't. Trust is the system everyone says matters and almost nobody actually trains. It's not soft. It's not optional. It's not psychology-versus-physiology. It's the system that decides whether the leg plants when the moment arrives — and a hesitant plant under sport load is one of the highest re-injury risk patterns we see.
Fear of re-injury is the single largest barrier to successful return to sport — and it lingers in athletes who are otherwise physically ready.
Your knee will not trust itself because the surgeon said it's healed, or because a calendar says it's been nine months. It will trust itself because you've given it thousands of reps of success — under increasing pressure — that prove to your nervous system the leg holds. The first time you fully commit to a cut in a real game, that confidence has to come from somewhere. Our job is to build it on purpose, in graded exposures, long before match day.
Elevated ACL-RSI / K-SES scores predict poor return-to-sport outcomes and increased re-injury risk independent of physical readiness. Kinesiophobia is not a personality trait — it is a treatable barrier with measurable predictors. Graded exposure, mastery experiences, observational learning, verbal persuasion, and physiological state management (Bandura's self-efficacy framework) all translate directly into ACL rehab. Treat it as a system, not a vibe.
Telling the athlete to "trust it." Confidence does not arrive by command. It arrives through successful exposures, in graded contexts, repeated until the nervous system stops asking the question.
Skipping psychological readiness assessment. ACL-RSI takes five minutes. K-SES takes less. Yet most clearance pathways never use them. Without a number, the conversation is opinion.
Big leaps in exposure. From rehab gym to full contact training in one jump is how confidence collapses. Each rung needs its own ladder — modified drill, full drill, modified game speed, full game speed.
Ignoring identity and meaning. Athletes lose part of who they are during a year out. Return-to-sport that doesn't address identity, relationships, and meaning leaves the most important system — the athlete — behind.
Trust is measured, planned, and trained — never assumed.

Key takeaway — Trust. The body is ready when the body is ready. The athlete is ready when the athlete is ready. Both need to be true. Both can be measured. Trust is data. Treat it that way.
Tool: ACL-RSI scores below 65 at clearance are a stronger predictor of second-injury risk than most strength deficits. Yet most pathways never administer it.
Watch for: The pre-plant glance. The half-committed cut. The leg that visibly searches for the floor. All measurable. All trainable.
Same program. Different week. Different result. Recovery doesn't happen in a vacuum — and pretending it does is how athletes plateau.
Two athletes can run the exact same rehab program in the exact same week and get completely different results. One sleeps eight hours, eats well, has manageable work and supportive family. The other is in exam season, sleeping five, training twice a day for a different sport, and dealing with a relationship break. Same program. Different week. Different outcome — and the difference has nothing to do with the program.
This is the system clinicians most often leave to chance. It's also the system that most reliably explains the "mystery" setbacks — the unexplained swelling, the plateau, the regression. Rehab does not happen inside the clinic. It happens inside the rest of the athlete's life.
Rehab capacity is not a constant. It is a variable — set every day by sleep, stress, nutrition, training volume, and life events. The same load is a different stimulus in a different week.
Think of your body's recovery capacity like a bank account. Sleep, nutrition, and downtime are deposits. Stress, work, study, life events and training are withdrawals. We can build a brilliant rehab program, but if your balance is in the red, your knee will respond accordingly. That's why we ask about your week, not just your knee. The week is part of the program. Sleep gets prioritised. Stress gets named. Training load gets adjusted. Sometimes the most important rehab session is the one we don't run.
Sleep restriction below 6 hours / night reduces muscle protein synthesis by ~18–20% and impairs motor learning consolidation. Chronic psychological stress elevates cortisol, drives systemic inflammation, and changes the recovery response to the same dose of training. Concurrent training load, school sport, off-program work, and life-event clustering must be tracked. Same prescription, different total load, different adaptation. Capacity is a moving target — treat it that way.
Ignoring sleep. Sleep is the single most modifiable lever in recovery. Untracked, it is the most common reason a program that worked last month stops working this month.
Treating life stress as outside the rehab remit. It isn't. Stress changes physiology, sleep, decision-making, and pain perception. It belongs in the assessment, the program, and the conversation.
Not auditing concurrent training. The athlete is also playing club, school, social, and general gym sessions. The rehab program is the visible load. The hidden load can be double.
Same dose, every week. The body is not a machine. Some weeks the prescribed load is right. Some weeks it's too much. Static prescriptions ignore the moving target.
Discharging at clearance with no life-load plan for sport season. Athletes return to a higher-load life than the one they rehabbed in. Without a transition plan, the new total load is the actual return-to-sport test — and it's usually the one that finds the gap.
We treat life-load as a system on the program, not noise around it.

Key takeaway — Life Load. The week is part of the program. Track it, name it, dose against it — or watch a perfectly designed rehab fail to land. You can't out-rehab a bad week. You can plan against it. Recovery happens in the rest of the athlete's life — or it doesn't happen at all.
Clinical note: "Most mystery plateaus aren't mysteries. They're the rest of the athlete's life showing up on the strength curve." — Matt · 20 yrs in clinic
Sleep note: Under 6 hours of sleep cuts muscle protein synthesis by roughly 18–20% and degrades motor learning. The cheapest training intervention there is.
Watch for: Unexplained swelling. Stagnant strength gains. "Off" week after a hard one. The week often contains the answer — ask about it.
The first 48 hours change almost nothing. The first 4 weeks change everything.
Almost every ACL athlete I meet is making one of three decisions in the first month — surgery, the Cross-Bracing Protocol, or rehab-first. The decision matters. The way it's made matters more. Here is how we think about it — honestly, with the evidence, and with the uncertainty that the evidence still holds.
A non-contact ACL rupture takes around 50 ms. Less than a blink. Foot plants, knee internally rotates and collapses inward, and the ligament fails before any conscious correction can happen. You don't outrun it. You don't out-think it. You pattern-train the conditions that make it less likely — or you don't.
What follows the moment is more important than the moment itself. Pain. Swelling. The pop. Then the choices begin — and most athletes are asked to make them inside seventy-two hours, with a swollen knee, an anxious family, and a calendar pressing in from all sides. Slow it down. The first decision is whether to rush the first decision.
Protect the joint. Reduce swelling. Restore quiet quadriceps activation. Get the leg straight. Walk if you can — weight-bearing as tolerated is almost always safer than the protective limp that builds in. Avoid making any irreversible decision under acute swelling and emotion. The knee is allowed a fortnight of grace before anyone has to choose a pathway.
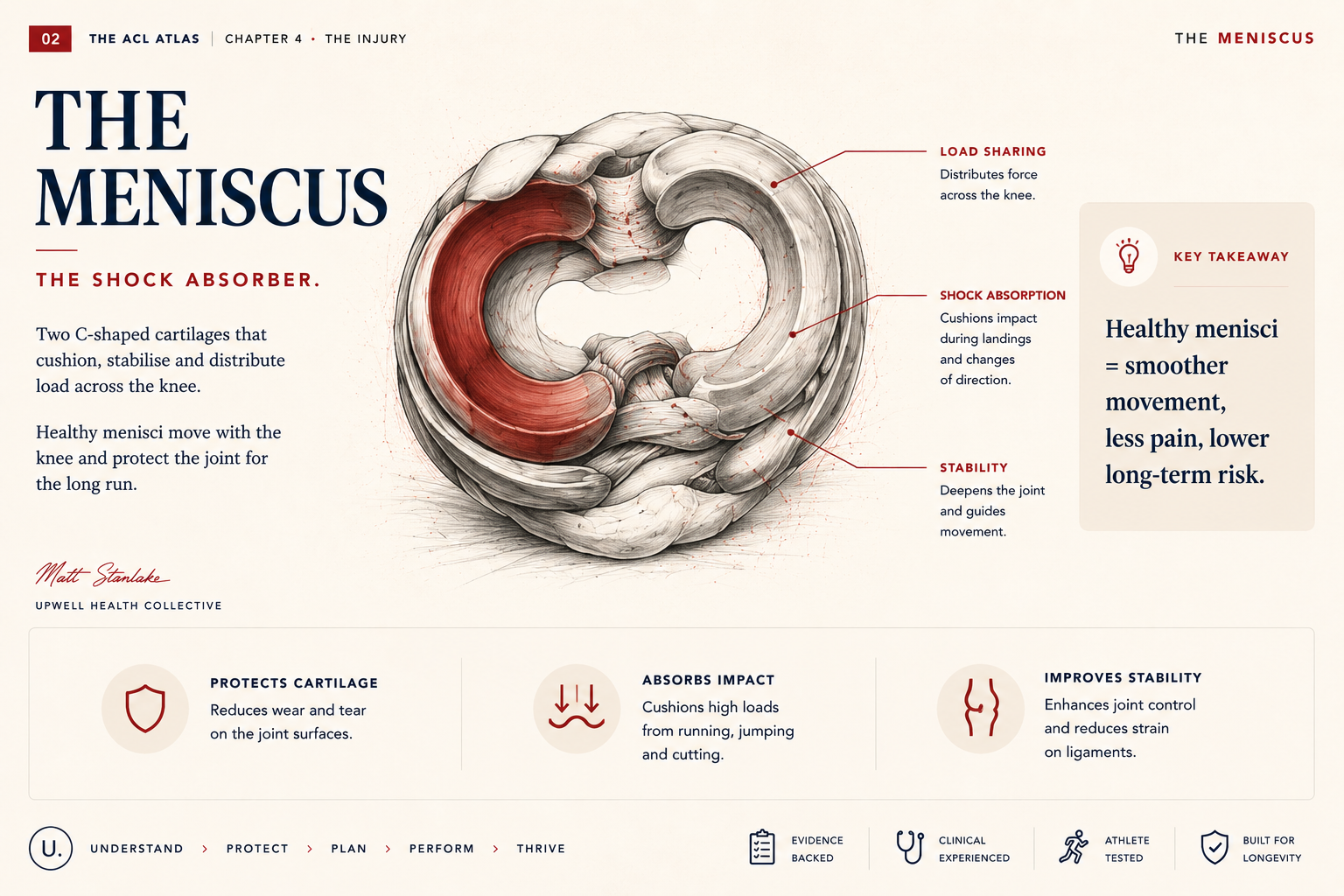
The meniscus is the unsung structure of the knee. ACL injuries that involve the meniscus have a fundamentally different recovery trajectory and a fundamentally different long-term joint health outlook. Preservation of meniscal tissue, when possible, matters more than most patients are ever told. A ramp lesion, posterior horn tear, or root avulsion changes the rehabilitation plan. It changes the loading floor. It changes the timeline. It changes the long-term osteoarthritis trajectory. The ACL gets the surgical headline. The meniscus often quietly decides what the knee looks like in ten years.
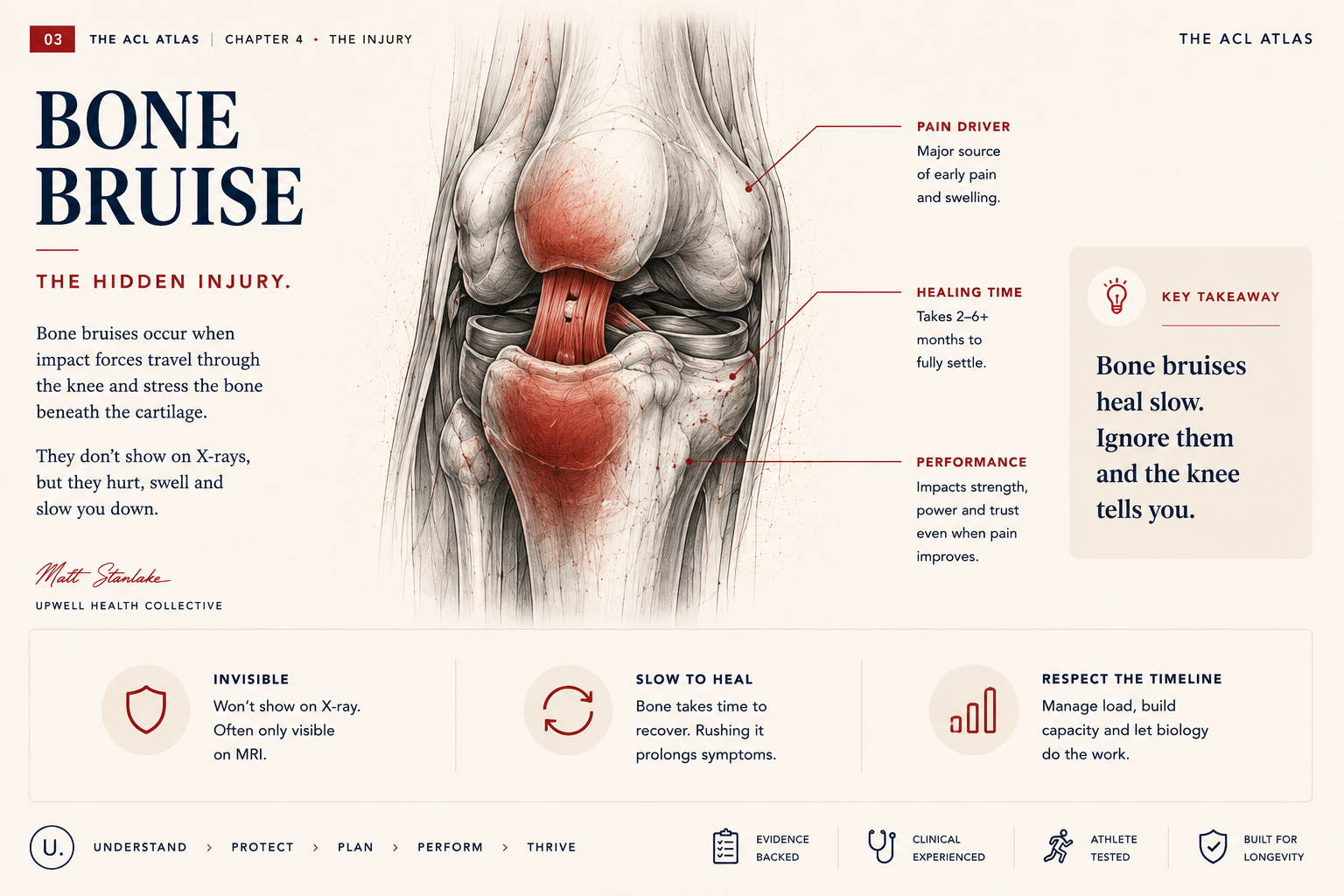
Bone bruising is the injury nobody talks about and almost every ACL patient has. The MRI shows it. The surgeon mentions it briefly. The patient is sent into rehabilitation without understanding that the bone bruise is often the source of pain weeks and months after the graft itself has settled. Bone bruise resolution can take six to twelve months. It changes loading tolerance. It changes early rehab. It changes return-to-running timing. Patients deserve to know about it — not as fear, but as context for why the knee aches in week 14 long after the surgical site has settled.
Three options sit in front of almost every ACL patient. They are not equivalent. They are not always available to everyone. And the right answer depends on the athlete, the sport, the concurrent damage, the surgeon's skill, and the family's capacity to support a year of rehab — not on the calendar of the next season.
Matt's take — first 48 hours. This is the decision most families rush. Don't. The knee gives you a fortnight of grace. Use it — for swelling to settle, for the MRI to be read properly, for the second opinion if you want one, for the surgeon conversation to be unhurried, and for the family to land somewhere together. The right pathway, chosen well, beats the fastest pathway, chosen under pressure.
The surgical gold standard for two decades. New ligament. Familiar pathway. Known timeline. Best fit: Pivoting sport athletes returning to high-demand cutting and contact. Concurrent injuries requiring surgical address. Recurrent giving-way despite optimal rehab. Young athletes with extended sport horizon. Trade-offs: 9–12 month rehab minimum. Graft donor-site morbidity. ~15–20% re-injury risk <2 yrs in young athletes. Post-traumatic OA risk over decades.
Bracing in deep flexion for 4 weeks to allow the native ACL to heal. Newer evidence. Strong early results. Best fit: Acute injury within 4–6 weeks. Tear pattern amenable to healing. Athlete able to commit to strict brace protocol. Willingness to accept newer-evidence pathway. Trade-offs: 4 weeks immobilised at 90°. DVT risk requires monitoring. Native ligament not always healable. Long-term outcomes still being studied.
No surgery, no brace — structured rehabilitation and a delayed surgery decision. Increasingly evidence-supported. Best fit: Lower-demand sport profile. Older athletes or recreational populations. No mechanical block to motion, stable on testing. Trade-offs: ~50% will still elect reconstruction within 2 yrs. Giving-way episodes risk further meniscus damage. Requires excellent rehab compliance.
What is well-established: ACL reconstruction restores rotational stability for pivoting sport. Rehab quality predicts outcome more strongly than graft choice. Concurrent meniscus injuries require timely surgical address when repairable. Psychological readiness (ACL-RSI) independently predicts return-to-sport success. Re-injury risk is highest in the first 2 years post-RTS, especially in athletes under 25.
What remains uncertain: Long-term CBP outcomes vs reconstruction in pivoting athletes — data still maturing. Optimal timing of surgery in acute-vs-delayed for various athlete profiles. Best graft choice for skeletally immature athletes. Whether prevention programs reduce contralateral risk post-RTS. True OA risk reduction with any particular pathway over decades.
The honest answer is this: no pathway eliminates risk. Every pathway has trade-offs. The best decision is the one made slowly, with the right team around the athlete, and with eyes open to what the evidence does and doesn't yet know.
Three main graft families. Each has a fit. None is universally better. Anyone who tells you otherwise is selling the technique they prefer — not the one that fits the athlete. The right answer depends on the athlete's sport, age, surgical history, donor-site tolerance, and the surgeon's skill with the specific technique.
Strength: Excellent · bone-to-bone fixation. Donor site: Anterior knee pain · kneeling discomfort. Best fit: Pivoting sport · contact athletes · revision surgery. Trade-off: Higher AKP risk in kneeling sports.
Strength: Comparable when properly fixed. Donor site: Hamstring weakness early · recovery often complete. Best fit: Kneeling sport athletes · smaller-frame athletes. Trade-off: Slightly slower bone–tendon integration.
Strength: Strong · rising in popularity. Donor site: Quadriceps weakness early · less AKP than BPTB. Best fit: Athletes wanting BPTB strength without the kneeling penalty. Trade-off: Surgeon-experience-dependent · newer technique.
Matt — what to ask your surgeon: "Which graft do you most commonly use for athletes like me, and why?" · "What's your re-rupture rate in this graft type?" · "If this is a high-risk profile, are we discussing LET / lateral augmentation?" The surgeon's answers tell you more than any graft comparison table ever will.
For young, female, or high-rotational-demand athletes, consider lateral extra-articular tenodesis (LET) or anterolateral ligament reconstruction in combination with ACL reconstruction. STABILITY trial evidence supports significant reduction in re-injury risk in this subgroup. Always a discussion to have with the surgical team. There is no single best graft. There is a best-fit graft for this athlete, this sport, this surgeon — chosen together, with the trade-offs understood.


Most ACL rehab is still graded on instinct. Looks good. Feels good. Probably ready. We use VALD™ force plates and dynamometry to replace probably with provably. Numbers don't make the clinical decision — but they stop the clinical decision being made on hope.
≥ 90% Limb Symmetry Index is the floor for return-to-sport on isokinetic strength. Achieved months before most athletes are actually ready. Symmetry alone is not readiness.
Matt — why we invest in this: Force plates aren't a gadget. They are the difference between "I think you're ready" and "here is exactly why we know you are." That sentence is the entire business case for the equipment, the testing protocols, and the time we spend reading the data with you.
01 — Isometric strength (IMTP · quad / hamstring dynamometry). Peak force production. Strength baseline. Floor metric. Target: LSI ≥ 90% + absolute N/kg target.
02 — Rate of force development (RFD at 100 ms / 200 ms). How fast force is produced. Sport speed signature. Lags strength by 6+ months. Target: LSI ≥ 90% within normative range.
03 — Eccentric capacity (Decel / Nordic / single-leg landing). Force absorption under load. Brake function. First to fail. Target: LSI ≥ 90% eccentric/concentric ratio.
04 — Reactive strength (CMJ · DJ · RSI). Stretch-shortening cycle. Predicts hop and cutting capacity. Target: CMJ asymmetry < 10%, RSI within normative.
05 — Repeatability under fatigue. Quality across multiple efforts. The first rep is not the test. Target: <10% drop-off, asymmetry stable.
06 — Single-leg propulsion (SL CMJ · SL hop). Limb-specific output. Bilateral can hide single-leg deficit. Target: LSI ≥ 90% per metric.
If you don't measure it, you can't earn it. And you can't prove it.
VALD doesn't replace clinical judgement — it sharpens it. The numbers become the language. The athlete sees their force profile, not just hears a verdict. The parent sees the trajectory, not just a vibe-based reassurance. The clinician makes the call against criteria, not against personality. Decisions stop being adversarial. And critically, when an athlete plateaus, the data tells us where. Strong eccentric but slow RFD? Train the RFD. Symmetric but absolute low? Train the absolute. Repeat-effort drop-off? Train the repeatability. The plateau stops being a mystery. It becomes a diagnosis.
Every six weeks, we re-test. You'll see exactly which metric is leading, which is lagging, what we're training next, and how close you are to clearance criteria. You stop being told you're ready. You see it. The athletes who return well are not the ones who feel ready. They are the ones whose profile says they are ready — across every dimension, against absolute and symmetric targets, under fatigue, at sport speed.

Most clinics still clear ACL athletes against a strength test, a hop test, and a calendar. We use a ten-layer readiness stack. Every layer must clear before sport. Skipping a layer is how the clearance test passes and the re-injury still happens.
Matt's take: The athletes who come back to me twelve months after a re-injury almost always cleared one test. Strong leg. Symmetrical hop. Surgeon happy. They were not un-cleared. They were under-tested. The stack is what under-testing looks like when you take it seriously.
Layers 1–6 · The six systems (Tissue, Force, Movement, Nervous System, Trust, Life Load)
L1 — Tissue. Biological readiness — graft phase, meniscus integrity, swelling history, surgeon clearance. Target: ≥ 9 months post-op, no effusion 4 wks.
L2 — Force. Full force profile clear — strength, RFD, eccentric, reactive, single-leg, all dimensions. Target: All metrics ≥ 90% LSI + absolute floor.
L3 — Movement. Landing, decel, cut clean at speed. Video + biomechanical screen at full sport pace. Target: Pass against criteria, inter-rater agreement.
L4 — Nervous system. Reactive control under demand — unanticipated cutting, dual-task drills, vision-restricted balance. Target: Reactive cut clean, dual-task stable.
L5 — Trust. Confidence under pressure — ACL-RSI scored, kinesiophobia screened, hesitation absent. Target: ACL-RSI ≥ 65, no pre-plant glance.
L6 — Life load. Capacity to sustain sport return — sleep, stress, schedule, total load all reviewed and managed. Target: Audit complete, plan documented.
Layers 7–10 · The sport-demand layers (where the systems meet the field)
L7 — Sport chaos. Knee holds in unscripted play — modified scrimmage, opponent pressure, full-speed reads. Target: Three sessions clear, no regression.
L8 — Fatigue. Movement holds when tired — quality maintained in last quarter of session, post-conditioning. Target: No drop-off in screen, no late-session symptoms.
L9 — Confidence under pressure. Athlete trusts the leg in moments — self-rated confidence under simulated match conditions. Target: Self-rated ≥ 8/10, coach-rated ≥ 8/10.
L10 — Decision quality. Sport intelligence intact — decisions read clean, body holds when the play breaks down. Target: Coach sign-off, match-tempo footage.
Cleared by every standard test. Not yet ready. Nine months post-op. Quad strength symmetric at 94% LSI. Single-leg hop clean. Surgeon green-lit return. The athlete felt good. The parents wanted the season. The club wanted the player back. By every common clearance criterion in Australian sport in 2025 — he was cleared.
We ran the stack. L2 force profile caught a 22% RFD asymmetry at 100 ms. L4 nervous system caught hesitation under unanticipated cuts. L8 fatigue caught a clear quality drop in the last quarter of repeat-effort testing. L9 confidence under pressure rated 5/10 self · 6/10 coach. He didn't go back to sport that month. We trained the deficits the stack revealed. Six weeks later, he cleared every layer. He returned, played the back-end of the season clean, and is still playing. The stack didn't hold him back. It told us what wasn't yet there.
"Symmetry on a hop test means I'm ready." Symmetry is one layer of one system. Both legs can be equally weak, equally hesitant, equally under-tested under fatigue. Symmetry lies on its own.
"It's been nine months. I should be cleared." Nine months is the floor for biology — not the ceiling for readiness. The stack tests against criteria. The calendar is permission to test, not permission to play.
"The surgeon said I'm good to go." Surgical clearance means the graft is healed and the joint is stable. That is layer one of ten. Surgeon clearance is necessary. It is not sufficient.
A knee can be 100% on the test and still 60% on the field. The stack is what closes the gap. Every layer cleared is a layer of risk closed. Skip a layer and the risk doesn't disappear — it just stops being seen. Readiness is not a moment. It is a stack — and a healed graft is not the same as a ready athlete.
The protocol that works for a 22-year-old male footballer is not the protocol that works for a 14-year-old female netballer, a 45-year-old recreational skier, or a 17-year-old gymnast with an open growth plate. Specifics change everything. Myths get athletes hurt. Here is what we know — honestly.
Female athletes rupture their ACLs at 2–8× the rate of male counterparts in matched sport. The reasons are multifactorial — hip-knee biomechanics, neuromuscular control under fatigue, hormonal cycle effects, and historical training differences. The reasons are not "weakness" or "fragility". They are training-modifiable factors that prevention programs consistently reduce by 30–50% when properly implemented.

Matt — the fragility myth: The 2–8× risk number isn't about female bodies being fragile. It's about movement patterns that haven't been trained for the demands of the sport. These are training-modifiable. The athletes I see who do the prevention work, properly and consistently, see their numbers come down. The protocols work. The barrier is implementation, not biology.
STABILITY trial subgroup data is increasingly clear: young female athletes returning to pivoting sport benefit from concurrent lateral extra-articular tenodesis (LET). Should be a default discussion in this cohort — not an afterthought.
.png)
Athletes with open growth plates need physeal-sparing surgical technique. Standard adult reconstruction can damage the growth plate and cause limb-length discrepancy. Always ask for the surgeon's paediatric experience. All-epiphyseal and partial-transphyseal techniques are well-described and outcome-proven in this group.
Matt — for parents of young athletes: Find a surgeon who operates on growing knees regularly. Not occasionally. Paediatric experience matters more than the brand of surgeon. Ask: how many under-16 ACLs do you do per year? What technique do you use for open growth plates? What's your follow-up protocol through puberty? Good answers exist. Demand them.
Reconstruction is not automatically the right answer in athletes over 40 who don't need to pivot competitively. Rehab-first pathways yield high-quality outcomes in this group, with surgery reserved for persistent instability or concurrent injury. The decision is sport-demand led, not age-led.
Matt — for recreational athletes 40+: Age is not a clinical category. I have 55-year-olds who pivot weekly. I have 25-year-olds who never will again. You are not your knee. You are someone who likes a particular kind of movement. The decision is about what you want to do, not what your driver's licence says you should want.
Myth: "You can't play sport without an ACL." Reality: plenty of athletes do, including at elite level — especially in non-pivoting sport. Function predicts viability, not anatomy alone.
Myth: "The graft is stronger than the original ACL." Reality: on day one yes, by lab measurement. By day 30, it's in remodelling and biologically weaker. By 12 months, it approximates a native ligament — but never fully replicates the sensory function.
Matt — where myths get athletes hurt: Half the athletes I see were given one of these as confident advice by someone they trusted. That's how myths get athletes hurt — not by the obvious bad ideas, but by the comfortable ones repeated by the right people. Read these once. Then read them once more.
Myth: "If I had surgery, I'm fixed." Reality: surgery rebuilds the ligament. Rehab rebuilds the athlete. The athletes who skip the second half are the athletes who re-injure.
Myth: "Bracing prevents ACL injury." Reality: functional bracing has not been shown to reliably prevent primary or recurrent ACL injury in pivoting sport. Neuromuscular training programs have. The cheap intervention beats the expensive one.
The athlete in front of us is a specific human, not a protocol. Specifics change the answer. Myths get in the way of the specifics.
ACL rehab is humbling and beautiful work. But the best thing we can do for an athlete is help them never need it. The evidence on prevention is strong, the cost is low, the implementation is the gap. Here is what works — and how we think about the long game beyond the first return.
~30–50% reduction in ACL injury risk when evidence-based neuromuscular prevention programs (FIFA 11+, PEP, Knee Control) are implemented consistently across a season. The cheapest intervention in the entire ACL story.
Three things, broadly. Neuromuscular control under load — landing mechanics, deceleration mechanics, change-of-direction quality. Strength foundations — hamstring strength, eccentric capacity, posterior chain. Movement variability under decision load — the ability to adapt mechanics when the play changes. Programs that train all three reduce risk meaningfully. Programs that only train one rarely move the needle.
The athletes who benefit most are the ones training prevention before they get hurt — which is the hardest sell in sport because nothing visible happens. The injury they didn't have is invisible. The training time invested is real. But the maths is overwhelming.
Min 0–6 · Part 1 — Running & activation. Forwards / backwards / sideways jogging through cones · hip-out, hip-in · circling partner · shoulder contact · quick forwards / backwards bursts.
Min 6–11 · Part 2 — Strength, plyometrics & balance. Bench (3 levels) · sideways bench · Nordic hamstrings · single-leg stance · squats · vertical / lateral / box jumps. The section most teams skip.
Min 11–15 · Part 3 — Running with cutting. Running across the pitch · bounding · quick sharp cutting · plant-and-cut at speed. Re-integrates the prevention work into sport-specific movement.
Run 2–3× per week, replacing the standard pre-training warm-up. Most of the 30–50% risk reduction comes from doing Part 2 properly — not skipping it for time.
Re-injury risk in the first two years post-RTS is meaningfully elevated, especially in athletes under 25, especially in female athletes, especially in contact and pivoting sport. The contralateral knee is also at elevated risk — the body has changed its movement strategy bilaterally, and the "good" side carries that change. Which means rehab does not end at return-to-sport. It continues, in lighter form, for years — as prevention, as monitoring, as ongoing neuromuscular training. The athletes who treat the first year back as maintenance rather than "rehab is over" are the athletes who stay back.
Post-traumatic osteoarthritis is a real risk after ACL injury — not because of the surgery, but because of the original trauma to the cartilage, meniscus, and bone bruise patterns that accompany most ruptures. The OA risk is reduced, not eliminated, by careful return-to-sport, weight management, ongoing strength training, and protection of the meniscus. The good news: the same things that make athletes good rehab athletes also make them good long-game athletes. Strength. Movement quality. Body awareness. Trust. Honest training. The Atlas is a return-to-sport guide — but more than that, it's a recovery system that pays out for decades.
For the parent — prevention isn't paranoia. If your young athlete plays a pivoting sport — netball, soccer, AFL, basketball, snowsport — integrated prevention training is the single best thing you can ask their team or coach about. It takes 10–15 minutes of every training session. It dramatically reduces ACL injury risk. It is not optional any more.
Rehab is what we do after. Prevention is what we do so most athletes never need the after. The athletes who win the long game don't stop training after the first return. They shift — from rehab, to prevention, to maintenance, to lifelong movement intelligence.
01 Injury. Acute care. Swelling down. Quiet quads.
02 Diagnosis. Imaging. Concurrent damage. Full picture.
03 Decision. Surgery. CBP. Rehab-first. Slow it down.
04 Prehab. If surgical. Full ROM. Quad activation. Calm joint.
05 Early rehab. Tissue respect. Loading floor. Foundations.
06 Strength. Absolute strength. Symmetry. Eccentric capacity.
07 Running. Linear mechanics. Volume. Quality at speed.
08 Plyometrics. RFD. Reactive strength. Landing skill.
09 Change of direction. Scripted cutting. Decel mechanics. Both sides.
10 Training. Modified team training. Cognitive load. Reactive.
11 Sport. Modified match. Full match. Stage by stage.
12 Performance. Sport demand met. Trust under pressure earned.
13 Maintenance. Lifelong. Prevention layer. The long game.
The pathway is not a staircase. From running back to strength when the engine isn't holding. From plyometrics back to movement when the chaos screen reveals a gap. From training back to trust when the body is there and the athlete isn't. The loops are not failure. They are the system catching what a linear protocol would miss.
If you only remember one thing from this Atlas, remember this: ACL recovery is not a timeline. It is a whole-athlete readiness problem. The athlete who returns well is the athlete whose six systems caught up to each other. Whose force profile cleared every dimension. Whose nervous system rebuilt its map. Whose trust caught up with their leg. Whose life made room for the work. Whose readiness was tested against ten honest layers — not one optimistic moment.
We have spent twenty years watching athletes return well — and watching athletes return badly. The difference is almost never courage. It is almost never effort. It is almost always whether the system in front of them was honest enough to test what mattered, and patient enough to wait for the data to say yes.
The Atlas is here so the difference between those two things is never left to chance.
This is not a guide written from fear. The athletes who come back well don't do it scared. They do it informed. Not chasing perfection, either — perfection is a bad target in any clinical decision. We are chasing better decisions, made by the right people, with the right evidence, at the right time.
The work we do now is not just for the next game, the next season, or the next clearance test. It is for the next forty years of the knee. The athlete who treats this twelve months as the first chapter rather than the whole story is the athlete who's still moving well at fifty — whose meniscus is protected, whose strength is preserved, whose movement intelligence compounds.
You will be the one who decides if you're ready. We will be the system that gives you the evidence to make that call honestly. Not perfect. Not fearless. Just clearer, calmer, and far less trapped by timelines than the day you walked in.
Welcome to the system. Welcome to Upwell.
If you or your athlete is navigating an ACL injury — fresh, post-op, mid-rehab, or back-but-not-quite-right — the Upwell Health Collective team in Camberwell sees ACL recoveries every week. Physiotherapy, exercise physiology, clinical Pilates, VALD ForceDecks testing, all under one roof. 28 free undercover carparks. All health funds accepted. Book online at upwellhealth.com.au or call (03) 8849 9096.
Matt Stanlake is the Head Physiotherapist and Director of Upwell Health Collective in Camberwell. He is a member of the Australian Physiotherapy Association (APAM) and AHPRA-registered (PHY0000975408) with 20 years of clinical experience. Matt has built Upwell into a 7x award-winning multidisciplinary allied health clinic trusted by AFL legends Mick Malthouse and Jonathan Brown. He is the author of Not Broken and the creator of the Whole Person Care™ framework.